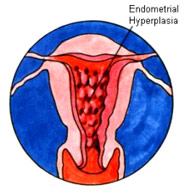
Endometrial Hyperplasia
Endometrial hyperplasia is an abnormal change in the
inner lining of the uterus that occurs most often to
women who are experiencing change of life, when there
is prolonged production of estrogen. Although endometrial
hyperplasia is benign, it may progress to a stage called
adenomatous hyperplasia. If you have this condition,
your chances of developing uterine cancer are increased.
The diagnosis can be confirmed by endometrial biopsy,
which is done in the office, or by dilatation and curettage,
commonly called a D & C. In either procedure, the
doctor scrapes tissue from the lining of the uterus,
which is then examined under a microscope by a pathologist.
If the tissue is found to be precancerous, removal of
the uterus will probably be recommended in order to
prevent the development of cancer at a later time.
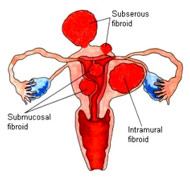
Leiomyomas or
Fibroids
When they cause pain, or profuse or prolonged menstrual
bleeding, put pressure on your bladder or rectum, or
begin to grow rapidly, they should be taken out. Although
nearly all fibroids are benign - noncancerous - on rare
occasions such rapid growth may indicate a malignant
change.
Removal of the uterus will solve the problem of troublesome
fibroids. If you are a young woman who may want to have
children and your fibroids are not too large or numerous,
you may be able to have a myomectomy, an operation in
which the fibroids are removed and the uterus is left
in place. This may not be a cure, however, because in
some cases new fibroids will grow, making further surgery
necessary.
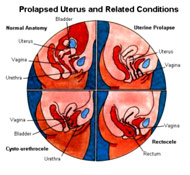
DEFECTS IN PELVIC
SUPPORTS
When the ligaments that hold your uterus in place are
weakened by childbearing or loss of elasticity due to
aging, they allow the uterus to drop from its original
positon down into and even through the vaginal opening.
This is called Uterine prolapse.
Similarly, the supportive tissues of the vaginal walls
may loose their elasticity, allowing the urethra, bladder
(urethero-cystocele) and rectum (rectocele) to bulge
out under the vagina.
By having you strain down during a pelvic examination,
your doctor can see the bulging of the vagina and how
far down the vagina the uterus has fallen. Urethro-cystocele
and rectocele can be treated by surgical repair that
restores the vaginal wall. Uterine prolapse can be treated
by removal of the uterus.
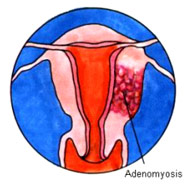
ADENOMYOSIS
If you have been having prolonged periods with heavy
bleeding, or pelvic or abdominal pain and tenderness
before, during, and after your period, your doctor may
suspect adenomyosis to be the cause. In this condition,
most common in women in their 40's, endometrial-like
tissue grows inside the wall of the uterus, making it
soft, enlarged, and tender.
The presence of adenomyosis can be confirmed only after
the uterus is removed and tissue from the wall is examined
under a microscope. The only effective treatment for
adenomyosis is removal of the uterus.
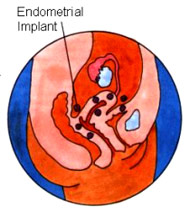
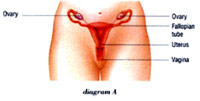
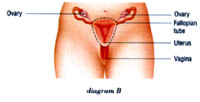
ENDOMETRIOSIS
The lining of the uterus is called the endometrium.
Cells similar to those that normally line the uterus
may also develop outside the uterus. This condition
is called endometriosis. These "implants"
attach themselves to the ovaries, tubes, bladder, rectum,
or other parts of the abdominal cavity, where they act
just as if they were the lining of the uterus - thickening
and bleeding each month according to your ovarian cycle.
Always benign, these implants may grow between one organ
and another, sticking them together with tight bonds
called adhesions. When endometriosis occurs in the ovaries,
blood-filled cysts often form endometriomas and can
cause considerable sudden pain and tenderness. Other
symptoms of endometriosis include premenstrual and menstrual
pain, prolonged or heavy periods, tenderness in the
lower abdomen, sharp stabbing pain during intercourse,
and lower back pain.
Because endometriosis is so closely tied to the ovarian
cycle, an absolute cure involves the removal of the
uterus and both tubes and ovaries. Depending on your
age and the spread of the disease, less extensive surgery
may be performed. If there are not too many implants,
it may be possible to remove them and leave the reproductive
organs in place. But as long as the ovaries continue
to function, new areas of endometriosis can arise.
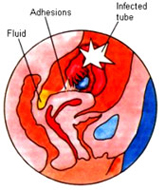
Pelvic Inflammatory
Disease
Pelvic inflammatory disease (P.I.D.) may be caused by
any one of a number of bacterial infections, including
gonorrhea. When acute infections of the tubes and/or
ovaries cause abnormal pain and tenderness, fever, and
a vaginal discharge, they are usually treated with antibiotics
and bed rest. If the infection responds to treatment,
the tubes will usually recover. But if the infection
was treated too late, or did not respond to antibiotics,
abcesses may arise that can rupture into the abdominal
cavity, causing peritonitis. This condition can be life-threatening,
and emergency removal of both tubes and ovaries as well
as the uterus may be necessary.
In Chronic PID, the moderate infection responded to
antibiotics, yet left you with permanent closed tubes
or adhesions in and around the tubes, leading to pelvic
and abdominal pain and painful intercourse. Depending
on the extent of the disease, it might be necessary
to remove both tubes and ovaries, as well as the uterus.