Miscarriage, often called spontaneous abortion, is
a loss of a pregnancy before 20 weeks. It occurs in
about 15 - 20% (1 in 6) of all pregnancies. Most happen
in the first three months, even before the woman knows
she is pregnant. Three or more consecutive miscarriages
may be called Recurrent miscarriage or Habitual abortion.
These women need special tests to try to find the
reason for recurrent losses.
After several miscarriages, you may wonder whether
you will ever be able to have a healthy baby. Be hopeful.
With treatment, the chances of having a successful
pregnancy are still good. Women with a history of
three or more consecutive miscarriages, but no live
births have a 50% of having a live baby in the next
pregnancy. However, if she has had at least one live
pregnancy, the chance increases to 70%.
CAUSES
The common causes include:
Genetic Causes
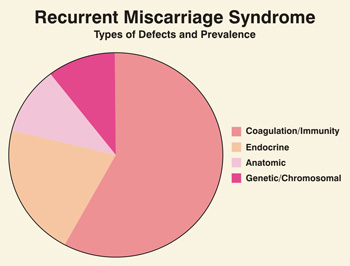
The major cause (50 – 60%) of early miscarriage
is probably a genetic factor. The most common genetic
defect resulting in miscarriage is an abnormal number
or structure of chromosomes. Often this is a nature’s
way of ending a pregnancy in which the fetus was not
rowing normally and would not have been able to live.
The numerical abnormalities are usually non-repetitive
(do not have an increased risk of recurrence in subsequent
pregnancies). The structural chromosomal abnormalities
are usually inherited from a parent with a balanced
translocation or inversion, and are repetitive.
In order to determine whether there is a genetic cause,
your doctor may order a karyotype on the fetal tissue
(obtained during a D&C) and on blood from both parents.
If the karyotype is abnormal, there is no therapy available,
but the information help explain the cause in these
patients. In about 5% of patients with recurrent miscarriage,
a balanced translocation or inversion is found in one
of the parents. If both parents have a normal karyotype,
it is likely that the miscarriage was a chance event,
and they should feel comfortable to plan a next pregnancy.
In cases of abnormal karyotype, genetic counseling to
discuss the degree of risk may be recommended.
Uterine Abnormalities
Approximately 10 – 15% of women with a history
of recurrent miscarriage have an abnormally shaped uterus.
The commonest example is a septate uterus, which involves
a central ridge or partition protruding into the uterine
cavity (Fig 1). Septate uterus occurs in about 3% of
women and about half of these have reproductive difficulties.
Other birth defects in uterine shape (congenital uterine
malformations) can likewise result in pregnancy loss.
IMAGE WILL HERE
One subset of women with uterine abnormalities is those
whose mothers took diethystilbesterol (DES) while pregnant.
DES women have a significantly higher incidence of miscarriage,
premature labor and infertility.
Uterine fibroids, especially those which grow in the
cavity (submucous fibroids) can distort the shape of
the uterine cavity can interfere with the implantation
or growth of the fetus. Fibroids can increase in size
during pregnancy and cause miscarriage.
These abnormalities can be easily diagnosed using high
resolution ultrasonography, a special x-ray called hysterosalpingography
(HSG), or by direct examination of the uterine cavity
using hysteroscopy (an endoscopic examination of the
uterine cavity).
The cervix can be congenitally weak or become weak due
to previous miscarriages or surgical trauma, unable
to support the pregnancy. About 20% of mid-trimester
(16 -20 weeks) pregnancy losses are caused by this condition,
called cervical incompetence. Once diagnosed, the subsequent
pregnancy can be carried to term by a surgical procedure
called cerclage or cervical stitch.
Hormone Imbalance
The luteal phase or the second half of the menstrual
cycle, is a critical time when the endometrium (lining
of the uterus) responds to the hormone progesterone,
which is produced by the ovary after ovulation. If the
progesterone production is low, infertility or miscarriage
can result. This occurs because the endometrium fails
to become a nourishing environment, preventing the embryo
from implanting securely. This problem is called the
luteal phase defect, which can result from abnormal
hormone levels or poor ovulation, and is easily corrected
by hormones (progesterone) or by correcting ovulation
using ovulation induction drugs.
Immunity Disorders
The immune system plays an important role in maintaining
health and responding to infection, injury or introduction
of foreign material. At this time, the immunologic interaction
between the mother and fetus is no clearly understood,
but it falls in two general categories.
The first category involves the production of certain
immunoglobulins or antibodies which the pregnant women’s
body creates and directs against circulating substances
that affect blood clotting. Examples of these antibodies
are lupus anticoagulant, anticardiolipids, and the antiphosholipids.
These antibodies affect fetal development, often resulting
in recurrent miscarriage. Therapy includes aspirin,
heparin or steroids in small doses. Although these mediations
may pose health risks, in selected cases, the pregnancy
outcome can be dramatically improved.
The second category involves an alteration in the immunologic
response of the mother against the pregnancy. During
a normal pregnancy, the fetus, which carries the father’s
foreign genes, survives in the mother’s uterus
because of a special protective response from the mother’s
immune system. In couples with recurrent miscarriage,
this protective response does not occur, and the maternal
immune system is activated to reject the (foreign) fetus.
Immunization (paternal leucocyte transfusion) to prevent
the maternal immune system from ejecting the fetus is
available.
Maternal Illness
Certain maternal diseases have been associated with
a higher rate of pregnancy loss. These conditions include
autoimmune diseases, thyroid disease, severe uncontrolled
diabetes, sere kidney disease and congenital heart disease.
Treatment of some of these diseases before conception
can improve chances for successful pregnancy.
Environmental
and lifestyle Factors
Smoking, drinking, and abuse drug use can increase the
risk of miscarriage. However exercise, working, intercourse,
travel and exposure to computer terminals do not increase
the risk of miscarriage. If couples are concerned that
their home or work environment may be hazardous, they
should consult their physician about this issue. Although
most medicines do not have an effect on pregnancy, there
are some which may be harmful and lead to miscarriage
and birth defects. Women should always consult their
physician before taking any medicines during pregnancy,
and also need to alert doctors or dentists before receiving
x-rays or prescriptions for medication.
DIAGNOSTIC TESTS
As recurrent miscarriage can be due to many possible
causes, your doctor will require a detailed history,
clinical examination, laboratory tests, x-rays, diagnostic
endoscopy to come to a working diagnosis.
These tests include:
- Complete blood count
- Thyroid and Diabetes screening
- S Progesterone assay
- Immunological tests (APTT, Lupus anticoagulant,
Anti-cardiolipin antibody, Anti-paternal antibody)
- Genetic study: karyotype of husband and wife
(in selected cases karyotype of products of conception)
- Ultrasonography
- Hysterosalpingography (HSG)
- Hystero-Laparoscopy and Endometrial biopsy.
Your doctor will decide which tests
to order, depending on the individual case. The treatment
will depend on the cause found.
WHAT YOU CAN
DO
- If you have had recurrent miscarriage, future
pregnancies should be planned, diagnosed early,
and watched carefully. You can improve your chances
of having a successful pregnancy in the future by
doing the following things:
- Having a complete workup before you
try to get pregnant again. The cause of the recurrent
miscarriage can be
found and treated.
- If you think you might be pregnant, see your
doctor right away. The sooner you seek care, the
sooner you can receive any special care you might
need.
- Follow your doctor’s instructions. He will
know how to keep yourself and your fetus as healthy
as possible.
|